The FDA is set to authorize “umbrella” clinical trials for rare diseases; the new approach will make the process faster and more sustainable by combining data from similar protocols, cutting redundant procedures, and reducing animal testing.
The coordinated effort that last spring saved the life of little KJ Muldoon earned widespread and enthusiastic media coverage. But between the invention of the treatment and its delivery to the patient lay a lesser-told story: an unprecedented manufacturing sprint. Genetic Engineering & Biotechnology News organized an online roundtable led by its deputy editor in chief, Julianna LeMieux, to discuss how therapeutic components were produced quickly, cost-effectively, and to clinical-grade standards.
The announcement was made yesterday at the annual meeting of the American Society of Gene & Cell Therapy and simultaneously published in the New England Journal of Medicine. I wrote about it for the Italian edition of Scientific American, but this story is worth seeing and reading. PS: Before KJ was treated for his metabolic disorder, there was the case of Terry Horgan, who had muscular dystrophy. Unfortunately, the personalized treatment for him came too late, and he did not survive an adverse reaction. So yes, we can say that KJ represents a first: the first time genome editing was used early, rapidly, and tailored enough to truly offer hope for a happy ending.
The progress of the new therapies of the CRISPR era can be told by interweaving two stories. The first is the one featuring Victoria, Carlene, Patrick, Alyssa, Terry and many others. There are over two hundred patients who have so far undergone some experimental treatment based on genome editing, i.e. the targeted correction of DNA instead of the addition of extra genes as in classical gene therapy. These women and men suffering from serious diseases had to face increasing pain and sacrifice until they decided to pin their hopes on a new type of experimental therapy, which is promising but not without risks. For the unluckiest of them, this act of courage and faith in science was not enough, but for many of these pioneers, life really did change. In fact, there are already dozens of people who have managed to free themselves (hopefully in the long term) from the burden of a rare genetic disease or, in some cases, leukaemia. Along with genetically edited cells, a new normalcy has arrived for them and the chance to finally think about the future.
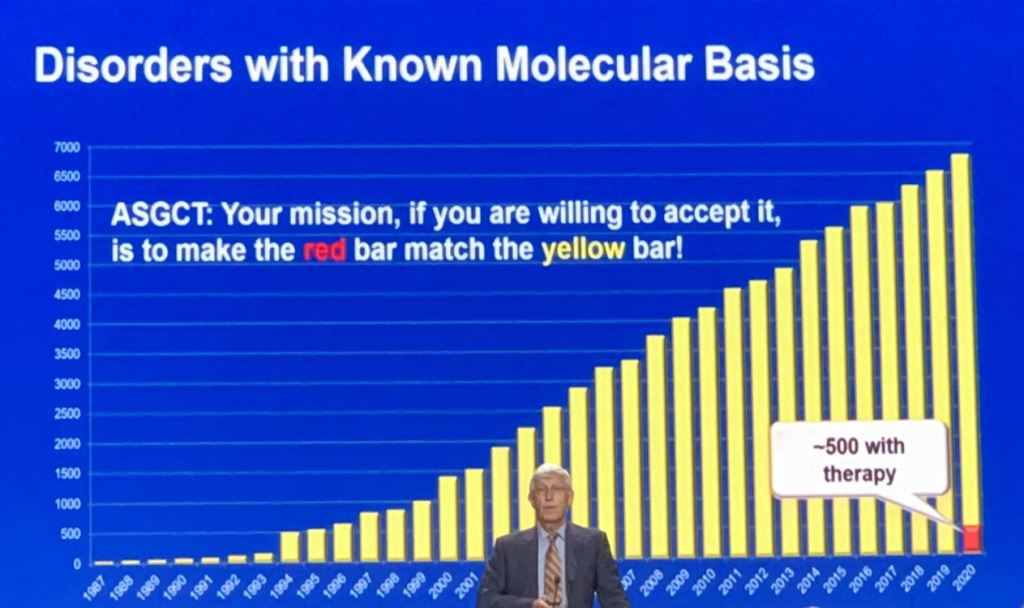
“Your mission is to make the red bar match the yellow bar”, urges a slide shown by Francis Collins at the annual meeting of the American Society of Gene & Cell Therapy held in Washington. There are almost 7,000 genetic diseases, but only about 500 with therapy. Most are not viable targets in a for-profit setting and won’t be managed by current gene-editing procedures. Hence the call to find something that is scalable. “We need a transformative approach.” Please read Kevin Davies’s account of the inspirational lecture given by the geneticist that led the Human Genome Project, then was appointed director of the NIH, and currently is Joe Biden’s scientific advisor.
Fyodor Urnov, University of California, Berkeley/Innovative Genomics Institute. Urnov is a pioneer in the field of genome editing, with a diverse background in academia, industry and the nonprofit sector. During his time at Sangamo Biosciences he co-developed and co-named human genome editing.
“Imagine CRISPR cures” is the title of the keynote by Fyodor Urnov at the World CRISPR Day conference on October 20. The talk was far from a celebration: “The fact that editing represents an approach to the majority of monogenic diseases in principle doesn’t mean that some biotech will take on disease number 823 in practice, and there are over 5,000 monogenic conditions on OMIM. Three years to IND in the best case scenario and cost scale of more than $6m per disease, that’s incompatible with either the promise of CRISPR to edit any given mutation which it can do or the unmet medical needs”. Don’t miss the on-demand video to learn more about the challenge of N=1 trials and Urnov’s call to arm against ultra-rare diseases.